How to perform acoustic reflex tests
Acoustic reflex threshold (ART) assessment
A survey performed in 2012 by Emanuel et al.1 indicated that two-thirds of American audiologists include acoustic reflexes in their standard test battery. Acoustic reflex tests measure the response of the intratympanic muscles to high sound pressure.
Contraction of these muscles increases the stiffness of the ossicular chain as well as the eardrum, although it is generally accepted that the acoustic reflex in humans is “mainly, if not exclusively, [due] to [the] contraction of the stapedius muscle”.2
The auditory activation of the tensor tympani muscle in humans occurs only as part of a startle response to extremely intense sounds. Acoustic reflex measurements can assist in the diagnosis of:
- Conductive hearing loss
- Retrochochlear lesion
- Neurological disorder
How to perform acoustic reflex tests
An acoustic reflex test can be performed ipsilaterally and contralaterally. In both cases, a probe is placed in the ear canal, presenting a constant 226Hz probe tone. Like tympanometry, this procedure enables us to measure any chance of impedance within the middle ear system.
As no pressure is used, short (around 10ms) and loud test stimuli are presented simultaneously to cause an impedance change. This is due to contractions of the stapedius muscle. The test signals used are typically 500Hz, 1, 2 and/or 4kHz at a range of 75 to 110 to 120dB. If the test signals are presented through the probe (in the same ear), the test side is performed ipsilaterally.
If another transducer is used to present the test signals to the opposite ear (e.g. the probe is placed in the left ear, and the transducer is placed in right ear), the test is performed contralaterally.
It is worth noting that different nomenclature exists in relation to ‘contralateral’. The Aural Acoustic Immittance Standard (ANSI) 19873 identifies contralateral as the side to which the stimulus is presented, e.g. contralateral right: stimulus in right ear, while the probe is placed in the left ear. Others consider contralateral with reference to where the probe is placed (e.g. contralateral right: stimulus in left ear, probe in right ear). With Amplivox tympanometers, the latter is used.
The physiology of acoustic reflex measurements
To interpret acoustic reflex measurements accurately, it is important to understand the physiological occurrences in the acoustic reflex arc. Afferent and efferent neurons work together to respond to an outside world stimulus. Afferent neurons carry information obtained by sensory receptors (in this case the ear) to the central nervous system (the brain).
As a reaction, efferent neurons transport the information away from the nervous system to the muscles (in this case the stapedius muscle) to perform an action. Research has shown that the stapedius reflex is the dominant sound-evoked pathway4, so that only the behaviour of the stapes muscles will be considered in this instance.
The auditory reflex arc is complex. High intensity stimuli reaching the cochlea stimulates the auditory nerve, which passes the information on to the ipsilateral VCN (ventral cochlear nucleus).
From here, the information is passed onto the facial nerve nucleus to trigger action in the motor neurons, which go to the stapedius muscle. As well as this, the information goes through the crossway pathways to the facial nerve nucleus of the contralateral ear, causing a contraction in the opposite stapedius muscle.
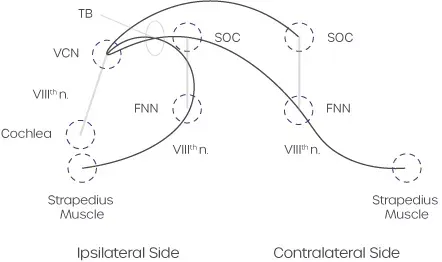
The stapedius muscle pulls the stapes posteriorly, causing the ossicular chain to stiffen when the stapes muscle is pulled away from the oval window. As a result, the middle ear admittance decreases, which can be measured in the outer ear canal.
Although the function of the middle ear reflex pathway appears to be protective, it has been proven that the reflex doesn’t provide sufficient protection against excessive stimulation5. Nevertheless, the contraction of the stapes muscle does result in a frequency-dependent sound attenuation.6
This minimises the masking of speech frequencies from intense background noise in order to preserve speech discrimination.7 Lastly, the stapedius may also contract to internally generate vocalisation and reduce self-stimulation.8
How to interpret acoustic reflex tests
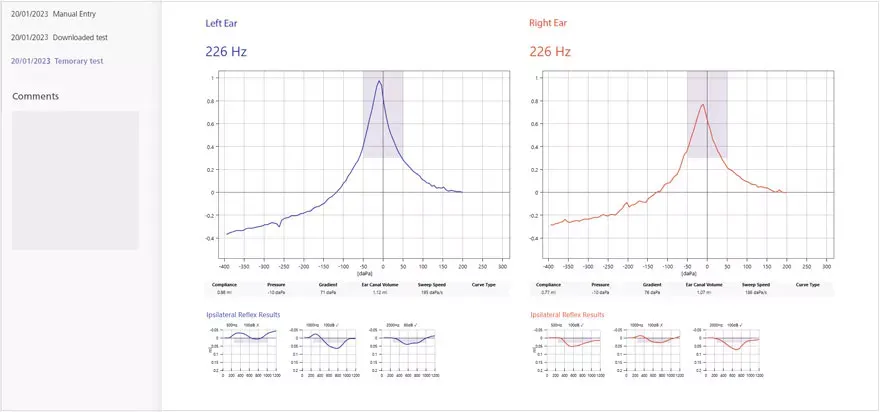
Acoustic reflex measurements are usually performed at 500Hz, 1, 2 and 4kHz, and measured both ipsilaterally and contralaterally at different intensities. Sometimes noise signals are also used (often when testing children). It’s quite common to perform quick screenings at one frequency and a single intensity, whereas diagnostic assessment includes several sound levels to review the entire threshold.
Typically, the ipsilateral acoustic reflex is measured at stimulus intensities of 70 through to 90dBHL.9 A normal contralateral threshold is around 5 to 10dB above the ipsilateral threshold. As well as reviewing the sound intensity at which the reflex is detected, the shape of the test curve gives evidence on the middle ear pathology.
This can include the magnitude of the deflection (e.g. 0.03ml required), contraction time, and the degree of the curve gradient at start and end point. It’s advisable to do a repeat presentation to confirm the reflex threshold.
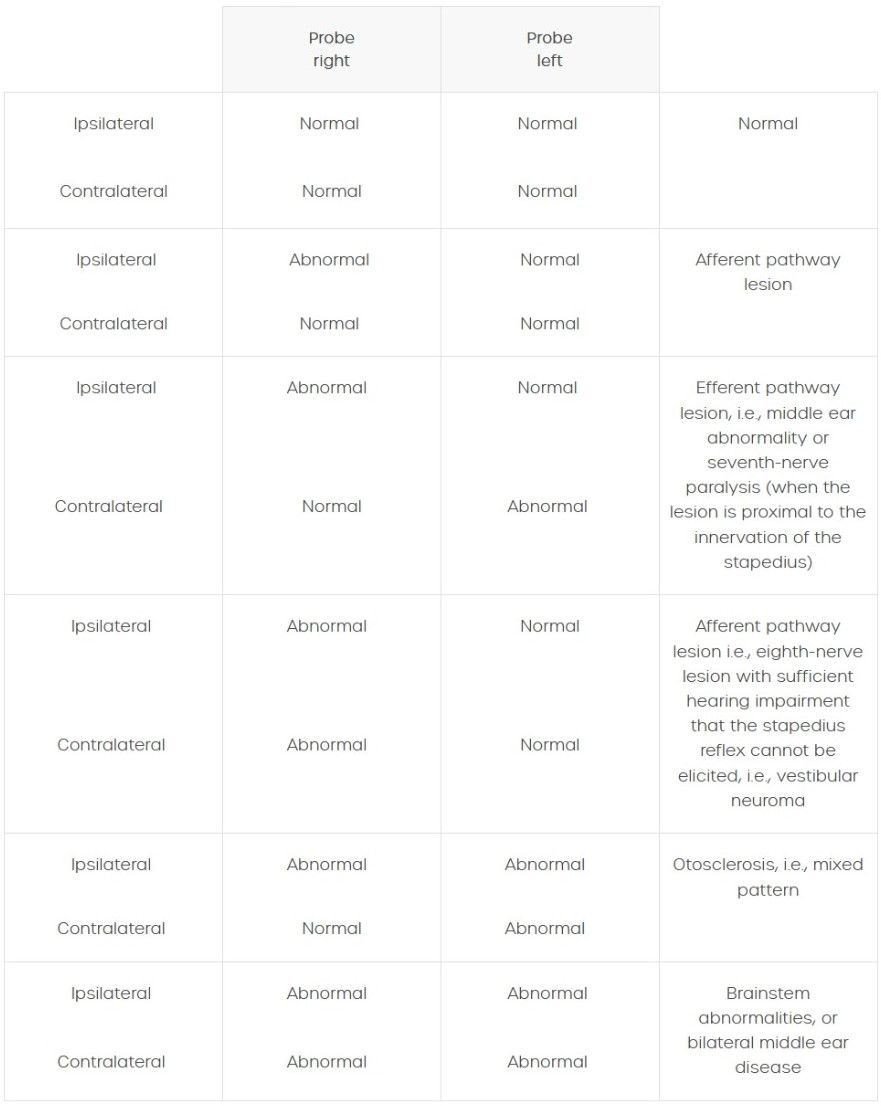
An overview of stapedius reflex threshold abnormalities can be found in the table below.10
Industry-leading tympanometers
Amplivox has worked hard to develop industry-leading handheld and desktop tympanometers that provide fast and accurate middle ear measurements for all age groups, including neonates.
With a compact and elegant design allowing for complete portability, our tympanometers are ideal for mobile use as well as clinical environments where space is at a premium. Including a wide range of test functionality, our devices ensure testing requirements can not only be met, but also exceeded.
For more information on our tympanometry products please visit our tympanometers webpage, contact our customer support team on +44 (0)1865 880 846 or email.